.png)

Contents
- What is endometriosis surgery?
- What are the types of endometriosis surgery?
- Who Needs Endometriosis Surgery?
- Endometriosis Surgery: How the Procedure Works
- What Happens After Endometriosis Surgery?
- Does Endometriosis Come Back After Surgery?
- Are There Any Risks to Endometriosis Surgery?
- Endometriosis Surgery and Fertility: What You Need to Know
- Book a Consultation with an Endometriosis Specialist via Amilis
- Frequently Asked Questions
In an eggshell...
- Laparoscopy (keyhole surgery) is the most common type of endometriosis surgery — and the gold standard for diagnosing endometriosis.
- Laparotomy is an open surgery option, usually reserved for more severe or complex cases.
- Surgery can significantly reduce pain and, in many cases, improve your chances of conceiving.
- Endometriosis can return after surgery — but the how and when depends a lot on how completely the disease is removed, its severity, and whether hormonal suppression is used afterwards
- Recovery is typically 1–2 weeks for laparoscopy, and 4–6 weeks for laparotomy
If you thought the waiting lists on the NHS were news enough, here’s a number that'll make you pause.
According to a recent report by Endometriosis UK, the average time to get an endometriosis diagnosis in the UK now stands at 9 years and 4 months- gone up from 8 years in 2020.
Additionally, nearly 40% of people visited their GP 10 or more times before endometriosis was even suspected.
That’s a wild statistic- especially when it translates to years of pain, dismissed symptoms, and zero answers.
And these just form the surface of what patients have to go through.
In the case you do get a diagnosis, figuring out what happens next — especially when it comes to surgery — can feel like a maze.
So we sat down with our medical team to gather all the info on endometriosis surgery, the types, how the procedure works and tips for recovery.
So, let’s go through it together 👇
What is Endometriosis Surgery?
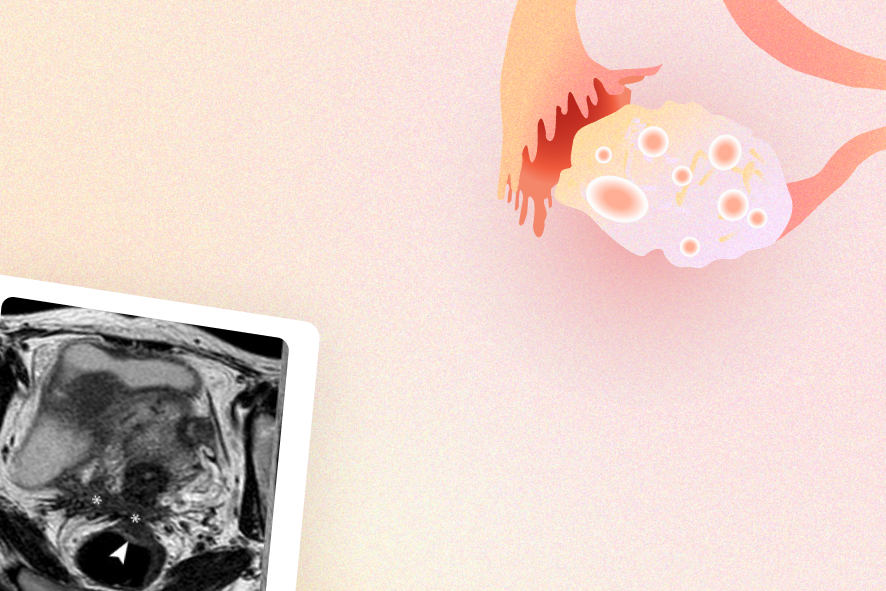
Endometriosis surgery is a procedure used to diagnose and/or treat endometriosis — a condition where tissue similar to the womb lining (endometrium) grows outside the uterus, usually on the ovaries, fallopian tubes, or pelvic lining.
"What happens in endometriosis is the lining inside the womb cavity migrates outside the womb” says Dr Xulin Foo, “One of the theories is something called retrograde menstruation, where the blood goes backwards through the tubes and deposits itself on the ovary or outside the ovary. It behaves like the lining of the womb — every time you have a period, it bleeds, it causes inflammation, it causes scarring."
Now, the point of surgery is two things:
1. To confirm the diagnosis 🔍
Endometriosis is one such condition that can’t be definitively diagnosed by scans or blood tests alone.
Turns out- visualising the tissue directly at surgery — ideally with a biopsy (a procedure where a sample of cells is taken from the uterine lining)— is the most definitive way to confirm it.
In fact, the majority of people are still diagnosed via laparoscopy. This is also why even if your scans come back normal, UK guidelines support offering surgery.
Okay, but is it a major surgery?
Well- It depends. For most people, endometriosis surgery means a laparoscopy — a minimally invasive, keyhole procedure that's done as a day case. One way to think of it is as a targeted, smaller-scale operation.
A laparotomy (open surgery), on the other hand-is the other option, reserved for more complex or severe cases.
We'll get into both below!
What are the Types of Endometriosis Surgery?
Laparoscopy (Keyhole Surgery)
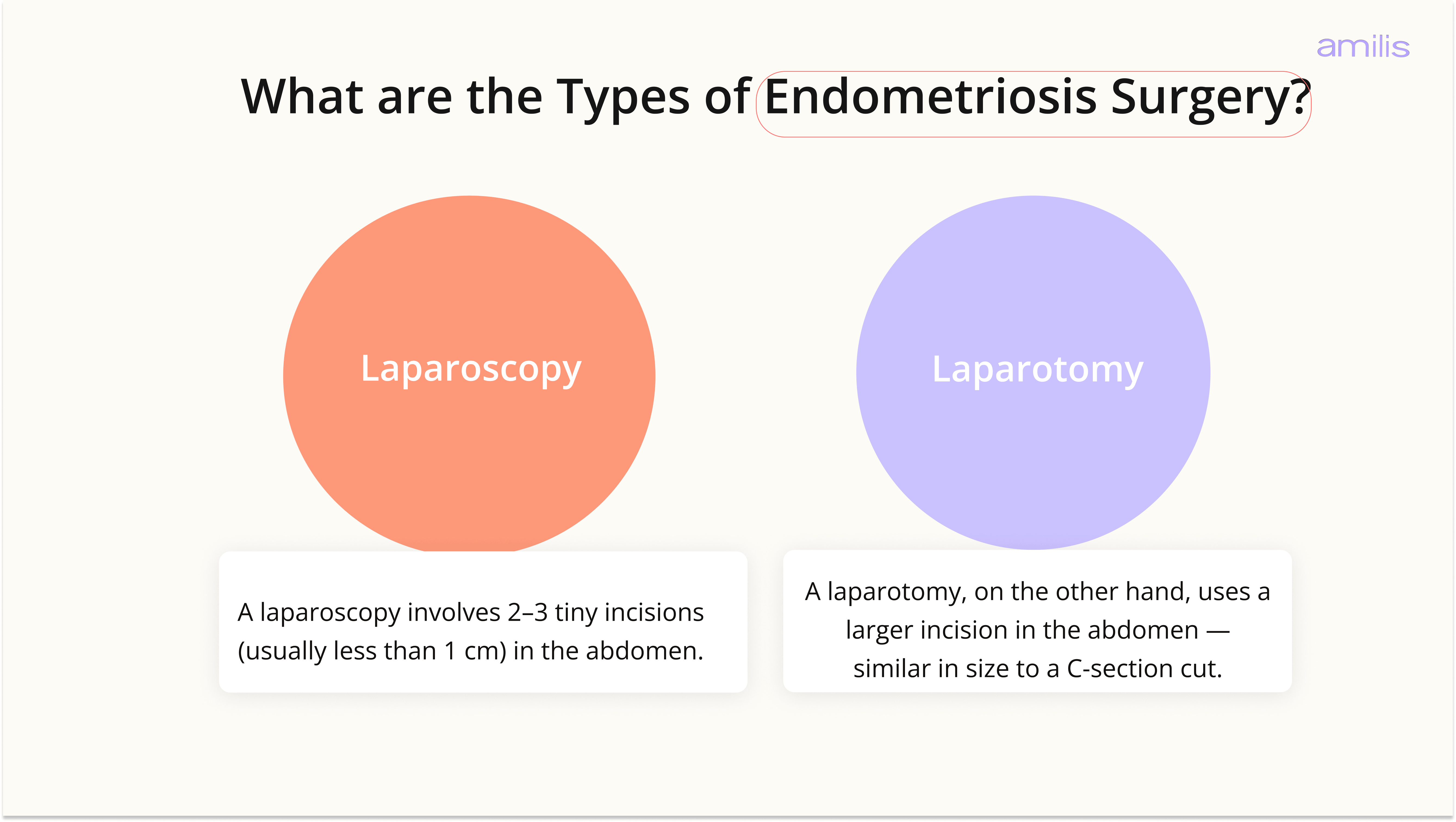
A laparoscopy is the most common — and preferred — approach to treat endometriosis.
It involves 2–3 tiny incisions (usually less than 1 cm) in the abdomen. A small camera (laparoscope) goes in through one incision, and surgical instruments through the others.
The surgeon watches these live images on a monitor and either:
- Ablates the tissue — burns or destroys it
- Excises the tissue — cuts it out completely
Sometimes both techniques are used, depending on where the lesions are and how deep they go.
The procedure is done under general anaesthesia and is usually a day-case or overnight stay.
Because the incisions are so small, scarring is minimal — we're talking 2–3 tiny marks.
Laparotomy (Open Surgery)
A laparotomy, on the other hand, uses a larger incision in the abdomen — similar in size to a C-section cut.
This gives your surgeon a clear, wide view and plenty of space to carefully handle tricky endometriosis spots.
It’s usually reserved for tougher cases where keyhole surgery (laparoscopy) just won’t work safely, such as:
- Endometriosis has spread to the bowel, bladder, or ureters
- There are large chocolate cysts (endometriomas) on the ovaries
- Previous surgeries have caused significant adhesions (scar tissue)
- Laparoscopic surgery isn't safe
But here’s the thing- Laparotomy is rarely performed today.
Thanks to improvements in keyhole surgery skills and tools (like HD cameras and precise instruments), most complex endometriosis—even deep or widespread cases—is now treated with tiny incisions.
Studies show these modern laparoscopies match or beat open surgery results for pain relief and fertility, but with way faster healing: you’re often home the same day, back to light activities in 1-2 weeks (vs. 4-6 weeks for open surgery), and left with just small scars instead of a long one.
Who Needs Endometriosis Surgery?
Not every endometriosis diagnosis requires surgery—but here’s when your specialist might recommend it:
If you Have Severe Pain Not Helped by Pills
If pelvic pain, painful periods (dysmenorrhea), or pain during sex (dyspareunia) keeps disrupting your life despite trying hormonal treatments — like the combined pill, mini pill, or a Mirena coil — Then surgery can get to the root of what's causing the pain.
As Dr. Xulin Foo, part of the Amilis medical team, puts it: "As gynaecologists, we generally recommend going on some kind of hormonal treatment first. But if despite medical treatments you are still experiencing increasing pain, then it might be time to think about surgery."
If pelvic pain, painful periods (dysmenorrhea), or pain during sex (dyspareunia) keeps disrupting your life despite trying hormonal treatments like birth control pills or IUDs, surgery can remove the root problem spots for longer relief.
If they Notice Growing Ovarian Cysts
“Chocolate cysts” (endometriomas) are blood-filled sacs on your ovaries that can grow large, twist, rupture, or affect fertility. In such cases, surgery drains and removes them to prevent complications.
If you are Trying to Conceive
If you’re trying to conceive and scans/tests point to endometriosis blocking eggs, tubes, or implantation, surgery clears these barriers to boost natural pregnancy chances (or improve IVF success).
If Endometriosis Has Spread to Other Organs
When endometriosis infiltrates bowel, bladder, ureters, or pelvic walls (deep infiltrating endometriosis), it causes issues like painful bowel movements or urination— and surgery precisely cuts it out.
If there’s a Need for a Certain Diagnosis
Laparoscopy lets doctors see and biopsy tissue directly—it’s the gold standard to confirm endometriosis (vs. symptom-based guesses).
Your doctor considers your age, pain levels, cyst size, family plans, and disease stage before suggesting it—so it’s always a collective decision tailored to you.
Endometriosis Surgery: How the Procedure Works
Here’s a clear step-by-step of what happens—from prep to recovery—so you know exactly what to expect. 📋
Before the surgery
Your team will walk you through what to do beforehand, but typically:
- You'll fast (no food or water) for 6–8 hours before the procedure
- Avoid perfumes, scented lotions, or deodorant on the day — these can release compounds that may affect the surgical environment
- Arrange for someone to drive you home and be with you for the first 24 hours post-op
- If deep endometriosis is suspected (especially involving the bowel), you may need a bowel prep beforehand
For more complex cases, your doctor may request additional investigations — like an MRI or contrast enema — to map out the disease and plan surgery properly.
During the procedure
For a laparoscopy, once you're under general anaesthesia, here's what happens:
- 2–3 small incisions are made in the abdomen
- A tiny camera is inserted to get a clear view of the pelvis and spot any lesions
- Surgical instruments are used to excise or ablate the tissue
- The cavity is flushed, and the incisions are closed
The whole thing takes anywhere from 30 minutes to 3 hours, depending on how extensive the endometriosis growth is.
In complex cases (think bowel or bladder involvement), there may be a colorectal or urological surgeon on the team, too.
What Happens After Endometriosis Surgery?
Right after surgery, you’ll be taken to a recovery area where the team keeps an eye on your breathing, pain, and vital signs.
Most people can go home the same day or the next morning, depending on how they feel and the type of surgery they had.
In the first few days, it’s very common to notice:
- Mild to moderate tummy discomfort or cramping
- Bloating, or a strange ache in the shoulder (this is from the gas used during laparoscopy and usually settles in a few days)
- Light vaginal spotting
- Feeling tired or “wiped out”
And here’s how long recovery might take in general:
- After laparoscopy (keyhole surgery): Many people are back to light daily activities in about 1–2 weeks, with most feeling fully recovered in 2–4 weeks.
- After laparotomy (open surgery): Healing takes longer, often around 4–6 weeks or more, especially if the surgery was extensive.
To help with recovery, short, gentle walks are usually encouraged soon after surgery to help with circulation and reduce the risk of clots.
Your doctor will usually ask you to avoid heavy lifting, intense exercise, and sex for a few weeks (often 4–6) until your body has had time to heal and you’ve been reviewed.
Lastly, a follow-up visit is normally planned around 6–8 weeks after surgery. This is when your specialist checks how you’re healing, goes over your results, and talks with you about pain, periods, fertility plans, and any next steps.
Does Endometriosis Come Back After Surgery?
The honest answer? It can.
Endometriosis can recur after surgery, particularly when the initial removal wasn't complete. In severe cases, recurrence rates after laparoscopy range from 18–29% in some studies, and in cases where no hormonal therapy is used afterwards, some research suggests rates can reach up to 50% within 5 years.
That said, recurrence isn't a given — and how thoroughly the disease was removed in the first surgery makes a big difference.
Complete excision (cutting out all visible spots) is associated with significantly lower recurrence than ablation (burning) alone, which is why the skill and experience of your surgeon really does matter.
A recurrence also doesn't mean you're back to square one. As Dr. Xulin Foo from the Amilis medical team puts it: "Even though you can't cure endometriosis, there are things you can do to prevent it from getting worse." Managing it long-term is very much possible — whether that's through hormonal treatments like the combined pill or GnRH therapy to keep it suppressed, or further intervention if needed down the line.
Are There Any Risks to Endometriosis Surgery?
All surgeries carry some risks, but serious problems are rare—especially with an experienced endometriosis specialist.
Here’s what to know in simple terms:
- Bleeding or accidental injury: Small chance of nicks to bowel, bladder, or ureters (tubes from kidneys)—your surgeon checks and fixes these right away if they happen.
- Infection: Mild risk at incision sites or inside; prevented with antibiotics and good care.
- Scar tissue (adhesions): Can form post-op and occasionally affect fertility or cause pain later.
- Anaesthesia side effects: Nausea or rare issues like breathing trouble—modern anaesthesia is very safe.
- Not all tissue removed: Leads to quicker regrowth (why excision by experts matters).
For deep endometriosis (affecting bowel/bladder), risks rise slightly, so these cases go to specialist centres with bowel/urinary teams for the safest results.
Endometriosis Surgery and Fertility: What You Need to Know
If you’ve been trying to conceive or are planning to, here’s what you need to know about endometriosis surgery:
Can surgery improve your chances of conceiving?
In many cases, yes. By removing lesions, endometriomas, and adhesions, surgery improves the environment in the pelvis — making it more favourable for conception.
Research shows that for women with endometriosis as their only fertility factor, pregnancy rates in some studies after laparoscopy were around:
- ~60% for minimal or mild disease (at 2–3 years post-surgery)
- ~50% for moderate disease
- ~40% for severe disease
Rates vary depending on age, disease stage, and other factors — but the general trend is clear: surgery can meaningfully improve your chances, with higher rates typically seen in milder disease.
For women with endometriosis in advanced stages, complete excision has been associated with spontaneous pregnancy rates of up to 60% within the first year after surgery. That's a significant outcome.
Does surgery affect egg quality or ovarian reserve?
This is where it gets a bit more nuanced. 🤓
Surgery near the ovaries — especially for endometriomas (chocolate cysts) — can affect your ovarian reserve. This shows up in tests like your AMH levels, and the more ovarian surgeries you've had, the more that risk builds up.
It also matters how the surgery is done. Some techniques, like excision with bipolar coagulation, are harder on the ovaries than others — plasma energy ablation or CO2 laser vaporisation tend to be gentler options.
So before any ovarian surgery, it's really worth having an open conversation with your surgeon about your fertility goals. A simple "I want to protect my fertility as much as possible — what's the safest approach for my ovaries?" is all you need to say. A good surgeon will take it from there.
Book a Consultation with an Endometriosis Specialist via Amilis
Waiting nearly a decade for a diagnosis is already too long.
At that timeline, we risk disease progression and battling with symptoms, which really shouldn’t be the norm for anyone.
At Amilis, we believe your well-being doesn’t deserve to be on a waitlist.
We’re here to help you figure out your options. Here's what you get when you choose healthcare via Amilis:
- Book Consultations with top-endometriosis specialists and gynaecologists across the UK — with little to no waiting times
- Get a detailed treatment plan as a part of your consultation, reducing time to diagnosis
- Book Free Consultations with vetted fertility clinics across the UK
And as always, you've got a stellar support team (that's us 👋) with you every step of the way.
Figuring out where to get started? Book a free call, or take our personalised fertility quiz to know more!
We're making healthcare accessible and affordable in the UK, one day at a time 💪🏻
Frequently Asked Questions
How long does a laparoscopy take?
It depends on what's being done. If the surgeon is just looking and confirming a diagnosis, it usually takes around 30–45 minutes. If treatment is carried out at the same time — removing or destroying lesions — it can take anywhere from 1 to 3 hours, depending on how much disease is found and where it is.
What is keyhole surgery for endometriosis?
Keyhole surgery is simply another name for laparoscopy. Instead of a large abdominal cut, the surgeon makes 2–3 tiny incisions — each under 1 cm — to insert a small camera and the surgical instruments needed. It's the most common approach for treating endometriosis, and because the incisions are so small, recovery is much quicker than with open surgery.
When should I consider surgery for endometriosis?
Surgery usually comes into the conversation when hormonal treatments aren't controlling your symptoms anymore, when ovarian cysts (endometriomas) are present, when advanced endometriosis is suspected, or when you're having difficulty conceiving. That said, it's always a decision made together with your gynaecologist, taking into account your symptoms, your stage of disease, and your personal circumstances and goals.
How fast does endometriosis grow back after laparoscopy?
It really varies from person to person, and it isn't guaranteed to come back at all. For mild to moderate disease where excision was thorough, recurrence may not happen for several years — or sometimes not at all. The single biggest factor is how completely the endometriosis was removed during the original surgery.
How do I deal with laparoscopy scars?
Laparoscopy typically leaves 2–3 small marks, each under 1 cm, and most of them fade significantly within 6–12 months. In the first few weeks, keeping the area clean and dry is the most important thing. After that, avoiding direct sun on the scars for around 6 months helps prevent them from darkening. Once the wounds are fully healed, silicone gel or scar sheets can help flatten and fade them further.